The growth plates produce longitudinal growth of the bone.
Growth Plate Anatomy
Growth plates are divided into layers or zones.
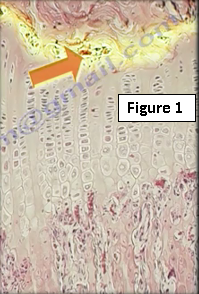
The reserve zone is inactive and allows for matrix production (Figure 1). It is used for storage and has low oxygen tension. It also has the highest type II collagen content.
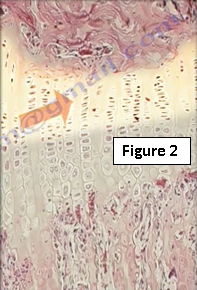
The proliferating zone is used for cellular proliferation and longitudinal growth, it has a high metabolic rate (Figure 2). This zone has the highest rate of extra-cellular matrix production and the highest oxygen tension.
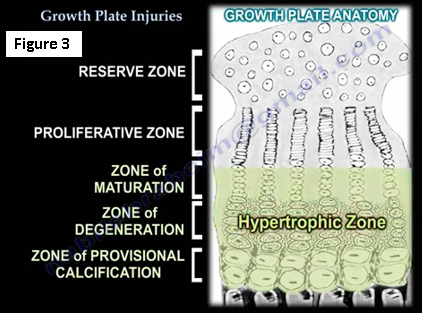
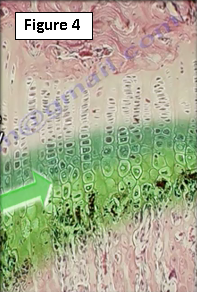
The hypertrophic zone is responsible for the zones of maturation, degeneration and provisional calcification (Figure 3). The cartilage cells increase 5-10 times in size. There is degeneration of the cells and the matrix is prepared for calcification. Regulation of chondrocyte maturation is controlled by hormones and growth factors. The parathyroid hormone inhibits chondrocyte maturation. Type X collagen is seen in the provisional calcification zone. Low oxygen tension, low vascularity, chondrocytes die and calcium is released for matrix calcification. The hypertrophic zone facilitates calcium depositions (Figure 4). The majority of growth plate injuries occur in the hypertrophic zone. This zone is weak and weaker than the ligaments and provides a cleavage pathway for the fracture.
Several classification systems of growth plate fractures have been developed and the most widely used is the Salter-Harris classification (Figure 5). Type I is a fracture through the growth plate, there may be no obvious displacement. Type II is a fracture through the growth plate and the metaphysis, sparing the epiphysis. Type III is described as a fracture through the growth plate and epiphysis, sparing the metaphysis. A Type IV fracture is one through all three elements, the growth plate, the metaphysis and the epiphysis. Type V is a compression fracture of the growth plate.

Salter-Harris Type I and Type II have a better prognosis than Types III and IV. In general, Types I and II may not require surgery, the reduction may be non-anatomic and the prognosis is usually good. Salter-Harris Type III and Type IV are intra-articular joint fractures that usually require surgery, the reduction has to be anatomic and the prognosis is fair. Type V is rare with a poor prognosis.
Contribution of Growth Plates to the Longitudinal Growth of the Bone
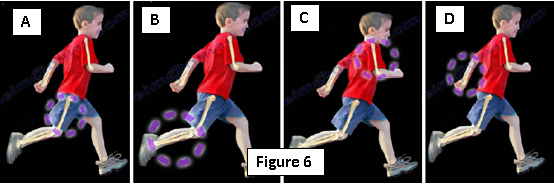
Here is a diagram to illustrate the contribution of the longitudinal growth (Figure 6). The proximal femur contributes to 30% of bone growth while the distal femur contributes 70% (6A).The proximal tibia contributes 55% of bone growth and the distal tibia contributes 45% (6B). The proximal humerus contributes 80% and the distal humerus contributes 20% of growth (6C). Lastly, the proximal ulna contributes to 80% of bone growth, while the distal ulnar contributes only 20% (6D).
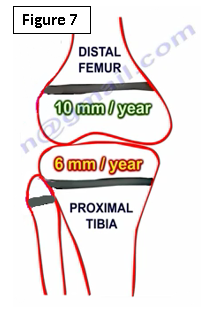
The distal femur contributes 10 mm of growth per year. The proximal tibia contributes 6 mm of growth per year (Figure 7). Girls complete growth at the age of 14 years. Boys complete growth at the age of 16 years.
Physeal Arrest
1.Total growth plate arrest occurs when the limb length decreases substantially (Figure 8).

2.Central: partial cessation of longitudinal growth causing progressive shortening (Figure 9). Physis bar or a bridge occurs in the middle of the physis. Less than 50% resection is done to allow growth of that bone.

3.Peripheral leads to angular deformity and decreased length (Figure 10). Corrective osteotomy and bridge excision.

Child Abuse and Growth Plate Injuries
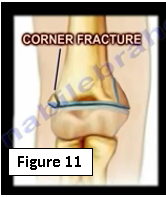
Usually you will find multiple fractures in different stages of healing. You will find physeal fracture or separation such as in the distal humerus. Transepiphyseal distal humeral fracture. A corner fracture is a traction/rotation injury pathognomonic of child abuse (Figure 11).
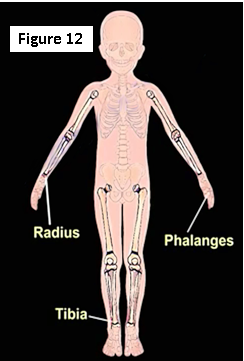
Fifteen percent of all fractures in children involve the growth plate, this occurs more in boys than in girls. These growth plate injuries occur more distal than proximal such as with the distal radius, distal tibia and the distal phalanges (Figure 12). Any fracture that involves the growth plate may create deformity and limb inequality. Doctors should discuss the risks with the parents.
For more information on growth plates, visit the links below:
https://www.youtube.com/watch?v=-eNJJRNxVRA
https://www.youtube.com/watch?v=JRc5Tss-RFI
For more information, visit my YouTube Channel:
https://www.youtube.com/user/nabilebraheim