By Susan Blumenthal, M.D. and Alexandrea Adams
The recent commemoration of National Women’s Health Week provided an important time to mark the progress that has been made in advancing women’s health over the past two decades and to highlight what more needs to be done to achieve women’s health equity in America. Historically, women have experienced discrimination in health care despite making 80 percent of health care decisions for their families, using more medical services than men, and suffering greater disability from chronic disease. Before the mid 1990’s, women were often excluded as subjects from medical research studies and underrepresented in the majority of clinical trials. Men were considered to be the “generic” humans in scientific studies, and the results from all male studies were then generalized to guide the diagnosis, treatment, and prevention of disease in women. Additionally, interventions to promote healthier lifestyles and prevent diseases like HIV/AIDS did not target women’s unique needs. Inequalities in health care limited women’s access to lifesaving diagnostic, treatment, and prevention services. Furthermore, many women paid more for their health insurance than men because of the possibility of pregnancy and their longer life expectancy (on average). This omission of women as research subjects and as the focus of prevention campaigns, as well as limitations on access to health care services had put their health at risk with rising rates of heart disease, diabetes, lung cancer, autoimmune illnesses, mental and substance use disorders, and the epidemic of AIDS.
I am proud to have played a leadership role in the 1990s as the country’s first Deputy Assistant Secretary for Women’s Health in the U.S. Department of Health and Human Services to write a new national prescription to improve women’s health in the Federal government, working with a broad range of partners in the public and private sectors in America and globally. The guiding principle of this prescription was that our country’s research, prevention, and service delivery programs must target all of the nation’s women—across all ages, socioeconomic, racial and ethnic backgrounds—addressing the health needs of the whole woman, in body, mind and spirit. Some of the actions that were taken during my tenure in the position include weaving a focus on women’s health into the missions of all U.S. health agencies, establishing National Centers of Excellence on Women’s Health at academic centers across the country to foster multidisciplinary research, increasing public education, enhancing health care professional training on sex differences in disease, and fostering the career development of women in medicine. I also established the National Women’s Health Information Center, which is a resource hub for comprehensive materials on a broad range of women’s health issues and the “Missiles to Mammograms” initiative that transferred imaging technology from the CIA, NASA and DOD to improve the early detection of breast cancer and others.
In 1993, as a result of powerful advocacy efforts, the National Institute of Health Revitalization Act was passed. This Act requires women and minorities to be included in clinical trials supported at the NIH as a requirement for obtaining funding. Just last year, a new NIH regulation was enacted to ensure that both male and female animals and cells were included in basic science studies and that findings were analyzed for sex differences. These transformational policies guide how research is to be conducted in the United States to help achieve women’s health equity.
The Patient Protection and Affordable Care Act of 2010 (ACA) legislation has also had transformational effects, adding an important element for advancing women’s health that had been missing for all too long—access to affordable, comprehensive health care. Prior to implementation of the ACA, there were 50 million uninsured Americans of whom 19 million were women. Women often paid more for insurance premiums than did men and were more likely to lose their insurance if divorced or widowed. In 2007, the number one cause of bankruptcies in the U.S. was lack of funds to pay medical bills. The American Journal of Public Health published a report in 2009 that estimated that 45,000 Americans died annually due to lack of health insurance. The United States was spending more than twice that of any other nation on health care but ranked 42nd on life expectancy and 37th out of 191 countries on the health status of our citizens. We were simply not getting what we paid for.
How the Affordable Care Act of 2010 (ACA) Improves Women’s Health
Signed into law on March 23, 2010, The Patient Protection and Affordable Care Act included multiple provisions to achieve an efficient, effective, and equitable health care system for both women and men. Since its implementation in 2012, the ACA has reduced the number of uninsured women by 9.5 million in the United States. Additionally, the legislation allows youth to remain on their parent’s insurance plan until age 26 which resulted in 7.7 million young women currently having health insurance. Another victory of the ACA is its inclusion of a “Patient’s Bill of Rights” which eliminates the gender rating of premiums. Insurance companies are now prohibited from charging women higher rates than men for similar coverage. Insurance companies also cannot deny coverage to those people who have pre-existing conditions which often prevented women who were pregnant, had cancer, a mental illness, or any other condition from obtaining insurance or paying much higher premiums. Furthermore, the ACA prevents insurance companies from instituting lifetime benefit caps, dropping patients who file reimbursement claims, and ensures that at least 80 percent of premium payments are spent on health care instead of administrative costs.
The ACA established Health Exchanges in states around the country for people who do not have employer insurance or qualify for Medicaid to purchase individual plans. Women whose incomes are between 100 and 400 percent of the Federal Poverty Level (FPL) are now eligible for tax-credits towards the purchase of insurance plans within the Marketplaces established by the law.
Importantly, the ACA significantly expanded eligibility for the Medicaid program, which insures low-income individuals at or below 138 percent of the FPL. 31 states and Washington, D.C. have accepted the Medicaid expansion provision of the legislation. Medicaid provides health insurance to more than 74 million Americans, among them 60% of nursing home residents and millions of disabled people. Currently, two-thirds of Medicaid beneficiaries are women. In 2010 Medicaid paid for 48 percent of all births, three quarters of all public family planning services, and provided supplemental coverage for nearly 1 out of 5 senior women on Medicare. The Medicaid expansion also included a provision for continuous coverage 60 days following the birth of a woman’s baby. Before the ACA’s Medicaid expansion, new mothers were ineligible in most states. The legislation has also helped women who do not have children obtain coverage.
The ACA mandates that all non-grandfathered insurance plans in the individual market and government health care plans must include ten Essential Health Benefits including ambulatory services, emergency services, hospitilization, maternity and newborn care, mental health and substance abuse services, prescription drugs, rehabilitive services, laboratory services, preventive and wellness services, and pediatric care. These comprehensive benefits are essential elements for improving women’s health.
The ACA emphasizes prevention as well as the treatment of disease. The United States spends $3.2 trillion on health care—18 percent of its gross domestic product (GDP)—but functions more as a “sick care” system rather than a “health care” system. In 2009, only 3-5 percent of the U.S. health budget was spent on prevention while 75 percent of medical costs were linked to the treatment of preventable lifestyle-related diseases. The ACA includes a provision that all insurance plans provide a range of preventive health services with no deductible or cost-sharing, including well-woman visits, pap smears, mammography, HIV testing, and cervical cancer screenings. Additionally, the ACA covers screenings and counseling for women who are victims of violence. The ACA also established the Prevention and Public Health Fund which allocated $18.75 billion for prevention services in communities and states including immunizations, heart health screenings, pandemic preparedness initiatives and other interventions. Incentives are included in the ACA for workplace wellness programs as well.
The ACA improves health care for women across the lifespan. It includes important reproductive health services for women. Contraceptives are covered as part of the basic package of no cost preventive services that insurers are required to provide with some exceptions given for religiously-affiliated organizations. The ACA also includes funding for a new education program that aims to inform teens about safe sexual practices and ensures that screenings for sexually-transmitted infections, including HIV, are readily available, especially for high-risk youth. The legislation helps pregnant women receive the care that they need. Although the United States is among the most advanced countries in the world, it ranks 136th in maternal mortality rate, having the highest maternal mortality rate in the industrialized world. To protect the health of mothers and babies, the ACA covers screenings for pregnant women for gestational diabetes, Hepatitis B, Rh incompatibility, HIV, and iron deficiency. Interventions to prevent birth complications due to alcohol consumption and tobacco use during pregnancy are also covered, as are folic acid supplements to prevent infant birth defects. Moreover, the ACA includes provisions to improve maternal and child health after birth by requiring coverage of breastfeeding support services, and workplace protections for nursing women. Postpartum depression (PPD) detection and treatment services as well as PPD research are included in the ACA. All of these interventions have important protective effects for both the physical and mental health of mothers and their children.
Furthermore, the ACA focuses on the special needs of women as they age. Women constitute 57 percent of the U.S. population over the age of 65, and 65 percent of the population over age 85. While women have a longer life expectancy than men (on average) and are at greater risk for chronic illness, women are less likely than men to have the financial resources to maintain their good health later in life. The ACA expands Medicare benefits—women constitute 59% of the program’s enrollees—covering preventive screenings for osteoporosis and other diseases, and providing a discount on prescription drugs for those who find themselves in the “donut hole”.
The ACA has also been a job creator in communities. With 20 million more people insured because of the legislation, the bill resulted in an increased demand for health care and the workers to provide it. The health care industry now employs 15.5 million people—5 million new jobs since the ACA legislation passed.
The American Health Care Act Will Reverse Progress in Women’s Health
With only Republican support, the U.S. House of Representatives passed the American Health Care Act (AHCA) on May 4th, 2017 to repeal and replace the ACA. This legislation is now being debated in the U.S. Senate.
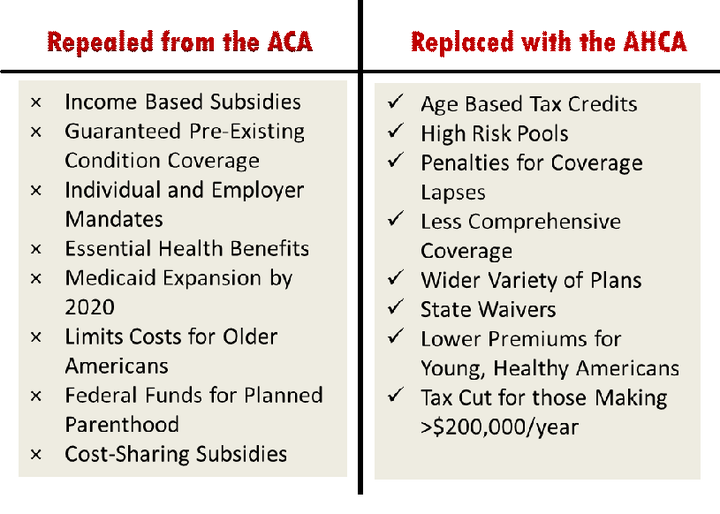
The AHCA eliminates many mandates, requirements, and funds provided under the Affordable Care Act of 2010 (ACA), providing states with greater autonomy about how they administer insurance coverage. Key AHCA provisions include eliminating individual and employer insurance mandates, ending Medicaid expansion, slashing tax subsidies that help low income Americans purchase health insurance, banning federal funding of Planned Parenthood, eliminating funding for the Public Health and Prevention Fund and allowing states to waive or modify the Essential Health Benefits package as well as eliminate the prohibition on charging people more for insurance if they have a pre-existing condition.

The House health reform legislation takes a machete to Medicaid, a program that provides health insurance for 74 million Americans—by cutting $834 billion of federal funds over ten years from the program. The President’s FY2018 budget proposes to cut an additional $610 billion from the program under the “pretext of reforming it”. When combined, according to a Center on Budget and Policy Priorities analysis, this represents an estimated 45% reduction in Medicaid by 2026, the largest restructuring of the program since its establishment in 1965. For most participants in the program, the federal government pays 50-75% of costs, depending on the state. Commencing in 2020, the AHCA would convert federal Medicaid funding from an open-ended matching system to an annual fixed amount of federal dollars provided to the states. States could select a “block grant” for payment of services for children under the age of 18 and low income parents of “dependent children” or a “per capita cap” approach for five population groups including seniors, people with disabilities, children of newly eligible adults, and all other adults. This capped approach will result in a reduction of federal spending, shifting the responsibility to states to pay more of the health care costs of its residents from their own budgets if they want to sustain Medicaid benefits at current levels. Women will be negatively impacted because they are a majority of Medicaid beneficiaries. Furthermore, with less money to spend on health care, state legislatures will have to make tough budgeting decisions that could take funds away from other programs that benefit women to pay for health services or reduce medical benefits. The AHCA would also set the level of tax credit assistance to purchase health insurance using primarily age and would repeal the ACA’s cost-sharing provisions for low income people. Women represent 54 percent of ACA marketplace enrollees in the 36 states that use the federally facilitated marketplace, healthcare.gov. An estimated 81 percent of beneficiaries in the health marketplace receive a premium tax credit, which offsets premium costs and makes health insurance more affordable. In 2015, more than 37 percent of women who purchased insurance were low income compared to 31 percent of men. Because women have lower incomes than men across all age groups in America, this provision of the AHCA could put women at a disadvantage compared to men and adversely affect their health.
The ACA has prohibited many discriminatory practices that were occurring in the individual insurance marketplace. While the AHCA maintains the gender rating ban and allows children to stay on their parents’ plan until age 26, it will permit states to allow insurers to charge higher premiums to individuals with pre-existing conditions. If the AHCA becomes law, states will be able to obtain a waiver from the U.S. Department of Health and Human Services (HHS) beginning in 2020 enabling insurers to charge women and men with pre-existing conditions higher rates. States can establish high-risk pools for insuring these people. The HHS has 60 days to review state waiver requests before they automatically go into effect. The AHCA includes an amendment that sets aside $8 billion to help states subsidize insurance premiums for people with pre-existing conditions. However, experts estimate that this is far too little to provide sufficient subsidies for all those who have pre-existing conditions. Women who are pregnant, have a history of mental illness, substance abuse, breast cancer or any other condition could be priced out of purchasing insurance coverage. Of particular concern is that women who are victims of any kind of violence will not be able to obtain coverage. Many assault survivors suffer from chronic conditions such as pain, gastrointestinal disorders, anxiety, depression, and post-traumatic stress disorder. Women with these conditions may have to pay more for their health insurance or might not be able to afford it altogether.
Furthermore, the AHCA makes insurance much less comprehensive by allowing states to obtain waivers to opt out of providing the Essential Health Benefits that are required under the ACA. All participating insurance plans, Medicaid and Medicare are required to cover ten categories of benefits. Those of particular importance to women have been the inclusion of maternity care, preventive services, and mental and substance abuse prevention and treatment. The elimination of the Essential Health Benefits takes our nation back to an era when women had a difficult time obtaining insurance with maternity coverage and other health services. Prior to implementation of the ACA, only 18 states had mandates for maternity coverage in the individual or small group insurance plan marketplace and there was no parity for coverage of mental and substance use disorders. While the AHCA would maintain preventive services requirements for private insurance plans, it will repeal the requirements for the Medicaid expansion. States could opt to roll back coverage for this population.
The Congressional Budget Office report released last week confirms that the AHCA would reverse the progress made in advancing women’s health care in recent years. The report estimates that if the AHCA is passed, 23 million people will lose their insurance by 2026, mostly as a result of the Medicaid cuts. Additionally, 1 out of 6 Americans will live in an area with an unstable non group insurance market. The report predicts that insurance premiums will rise for low-income, older Americans by as much as 9 times the current rates. The CBO report also underscores that most Americans will obtain less comprehensive coverage due to the elimination of the Essential Health Benefits provisions contained in the AHCA. While the AHCA would lower premiums for the young and the healthy, it will take away many people’s access to comprehensive medical services.
Contraceptive coverage is jeopardized for women in the AHCA. The bill defunds Planned Parenthood (PP), an organization that serves 2.5 million women annually. 6 in 10 women who use PP report it as their primary source of health care. 75 percent of PP’s patients are 150 percent below the FPL. PP has begun to close its doors in some states due to legislation that eliminates funding for the organization. Without federal dollars, PP will not be able to serve the 14,676 patients who have been affected by the closure of 10 health centers in the Midwest and Southwest. As a result, women will have less access to contraceptives, family planning and counseling, and cancer and STI screenings.
What actions can be taken to strengthen the Affordable Care Act?
Many health experts believe that the ACA should be repaired instead of repealed and replaced. What are some of the strategies to accomplish this goal? First, Medicaid should be expanded in states that have not yet done so and raise the income level for qualifying so that more people are eligible to enroll. The Federal government could also provide more funds to lower the cost of health insurance that individuals and families face. This could be accomplished in part by increasing the level of subsidies available for insurance plans purchased on the exchanges, or raising the income thresholds at which the subsidies phase out—or both. Strategies are needed to get more healthy people to purchase insurance including considering an automatic insurance enrollment procedure. With more healthy people in the risk pool, insurance premiums would be reduced. Private insurance markets only work well when there is a large and diversified risk pool. If they are going to provide universal or near-universal coverage, the individual mandate will have to be enforced which may mean raising the penalties for non-compliance and enforcing them more effectively. A public option, “A Healthy USA Plan” and/or lowering the age for enrollment into Medicare might also be considered as ways to get more people insured. Additionally, there is $8 billion in reinsurance payments that have been promised to insurance companies under provisions of the ACA that could help bring premiums down but have been blocked by Republicans. Drug prices should also be better negotiated. America is the only country in the industrialized world that does not contain rising pharmaceutical costs in this way.
Sadly, the Administration’s proposed FY2018 budget (A New Foundation for American Greatness) does the opposite of strengthening the ACA. While it proposes to eliminate the country’s budget deficit, instead the budget provides major tax cuts to the wealthy at the expense of the sick and the poor. The Tax Policy Center estimates that the top 1% of wage earners would receive a $37, 500 tax cut annually while the middle class would get about a $300 tax cut. The Administration’s budget proposes significant cuts to Medicaid and the Children’s Health Insurance Program (CHIP) over the next ten years and prohibits any federal funding for Planned Parenthood. The FY2018 budget also includes a $192 billion cut from the Supplemental Nutritional Assistance Program (SNAP) which will negatively affect 40 million low income Americans, 50% of whom are children. It also reduces the Centers for Disease Control and Prevention (CDC) budget by 17 percent, significantly impeding efforts to build a culture of health in America and jeopardizing public health preparedness initiatives to help prevent and respond to infectious disease outbreaks in the United States. Additionally, the budget includes a $6 billion cut for the National Institutes of Health (NIH) which would seriously thwart efforts to discover cures and prevention strategies for the diseases that affect women and men in our country today.
The bottom line: the ACA of 2010 significantly reduced the number of uninsured women in America, providing tens of millions of people with comprehensive health services, a patient’s “Bill of Rights” that prohibits discriminatory insurance practices, and has begun a prevention revolution as a result of many provisions contained in the law. Under the AHCA, an estimated 23 million people will lose their health insurance by 2026. American women will get sicker again. The ACHA will cut taxes for the wealthy but have devastating effects for the health of Americans as well as for the budgets of state governments, hospitals and public health programs. We can and must do better as a nation.
Summary
Over the past 25 years, much progress has been made to advance women’s health. As a result of the passage of the ACA, a critical ingredient was added to the national prescription to improve women’s health that had been missing until recently—access to comprehensive, quality health care. The ACA contains provisions to address the unique needs of women across their lifespan.
Recent debate has focused on repealing and replacing the ACA instead of strengthening the law. The passage of the American Health Care Act (AHCA) earlier this month in the U.S. House of Representatives eliminates the expansion of Medicaid by cutting almost $1 trillion from the program over the next ten years, removes subsidies to purchase insurance for low income Americans, blocks Planned Parenthood from receiving Medicaid reimbursements, allows states to eliminate Essential Health Benefits and charge higher insurance premiums for people with pre-existing conditions, and cuts critical prevention and preparedness funds. Since access to comprehensive health care is a key element in the prescription for women’s health equity, we all have much at stake in the current debate over the future of America’s private and public insurance programs.
Nobel Prize winner, Madame Marie Curie, once said, “I never see what has been done. I only see what remains to be done.” Let us resolve to do what remains to be done to strengthen the Affordable Care Act, increase investments in medical research, and emphasis the power of prevention to ensure a healthier future for all women—and men—in the United States.
Rear Admiral Susan J. Blumenthal, M.D., M.P.A. (ret.) is the Public Health Editor of the Huffington Post. She is a Senior Fellow in Health Policy at New America, a Clinical Professor at Tufts and Georgetown University Schools of Medicine, and Senior Policy and Senior Policy and Medical Advisor at amfAR, The Foundation for AIDS Research. Dr. Blumenthal served for more than 20 years in senior health leadership positions in the Federal government in the Administrations of four U.S. Presidents including as the first Deputy Assistant Secretary of Women’s Health, Assistant Surgeon General of the United States, and as Senior Global Health Advisor in the U.S. Department of Health and Human Services. She also was a White House Advisor on health. Prior to these positions, Dr. Blumenthal served as Chief of the Behavioral Medicine and Basic Prevention Research Branch and Chair of the Health and Behavior Coordinating Committee at the National Institutes of Health (NIH). She has chaired numerous national and global commissions and conferences and is the author of many scientific publications. Admiral Blumenthal has received many awards including honorary doctorates and has been decorated with the highest medals of the U.S. Public Health Service for her pioneering leadership and landmark contributions to advancing health in the United States and worldwide. Named by the New York Times, the National Library of Medicine and the Medical Herald as one of the most influential women in medicine, Dr. Blumenthal was named the 2009 Health Leader of the Year by the Commissioned Officers Association and as a Rock Star of Science by the Geoffrey Beene Foundation. She is the recipient of the Rosalind Franklin Centennial Life in Discovery Award.
Alexandrea Adams is a junior at Dartmouth College studying Biology and Public Policy. She is currently a Health Policy Intern at New America in Washington D.C.
References:
[1] U.S. Department of Labor. “Fact Sheet - General Facts on Women and Job Based Health.” 10 Oct. 2012.
[2] Cecere, D. "New Study Finds 45,000 Deaths Annually Linked to Lack of Health Coverage." Harvard Gazette. 06 May 2017.
[3] "World Health Organization Assesses the World's Health Systems." WHO. World Health Organization, 2017.
[4] "Country Comparison: Life Expectancy at Birth," Central Intelligence Agency, 2016
[5] H.R. 3590, 111th Cong., U.S. Government Printing Office (2010) (enacted).
[6] "Health Reform: Implications for Women’s Access to Coverage and Care." The Henry J. Kaiser Family Foundation. 29 August 2013.
[7] "Health Insurance Coverage and the Affordable Care Act." ASPE. 05 May 2015
[8] Centers for Medicare/Medicaid. Reducing Costs, Protecting Consumers: The Affordable Care Act on the One Year Anniversary of the Patient’s Bill of Rights, 2011.
[9] Centers for Medicare/Medicaid. National Health Expenditures 2015 Highlights. 2015
[10] Blacksher, E, "Health Reform: What's Prevention Got to Do with It?" Hastings Center Report, vol. 39 no. 6, 2009
[11] Partnership to Fight Chronic Disease and Partnership for Prevention. The Value of Prevention.
[12] "Prevention and Public Health Fund." HHS.gov. US Department of Health and Human Services, 16 Dec. 2016.
[13] Norris, L. "How Obamacare Changed Maternity Coverage." Health Insurance Resource Center. 16 Aug. 2016.
[14] "Country Comparison: Maternal Mortality Rate," Central Intelligence Agency, 2010
[15] Wong, R. and Palloni, A. "Aging in Mexico and Latin America." International Handbook of Population Aging (2009): 231-52.
[16] "Our Time is Now" The GOP's New Health Care Plan. 04 May 2017
[17] The Editorial Board, "Trumpcare’s Cruelty, Reaffirmed." The New York Times, 27 May 2017.
[18] Mangan, D. "24 Million Would Lose Health Insurance Coverage under GOP's Obamacare Replacement by 2026." CNBC. 14 Mar. 2017.
[19] Ranji, U., Salganicoff, A., Sobel, L., and Rosenzweig, C. "Ten Ways That the House American Health Care Act Could Affect Women," The Henry J. Kaiser Family Foundation. 08 May 2017.
[20] "Marketplace Plan Selections by Gender," The Henry J. Kaiser Family Foundation. 09 Dec. 2016.
[21] Levitt, L., Damico, A., Claxton, G., Cox, C., and Pollitz. K, "Gaps in Coverage Among People With Pre-Existing Conditions." The Henry J. Kaiser Family Foundation. 17 May 2017.
[22] Somashekhar, S. "Planned Parenthood to Close 10 Health Centers across Midwest, Southwest." The Washington Post, 19 May 2017.
[23] "National Women's Health Week." Womenshealth.gov. 10 May 2017.
[24] Office of Management and Budget. "Budget of the U.S. Government: A New Foundation For Greatness." 23 May 2017
[25] Achenbach, J., and Sun, L. H. "Trump Budget Seeks Huge Cuts to Science and Medical Research, Disease Prevention." The Washington Post. 23 May 2017.
[26] Davis, J. H. "Trump’s Budget Cuts Deeply Into Medicaid and Anti-Poverty Efforts." The New York Times, 22 May 2017.
[27] Blumenthal, M.D., S. "Healing America's Health Care System." The Huffington Post. TheHuffingtonPost.com, 03 Aug. 2012.
[28] Blumenthal, M.D., S. "Women's Health: Decades Later, What's Still Neglected." The Huffington Post. TheHuffingtonPost.com, 08 Mar. 2011.