

A patient takes a dose of methadone at an opioid treatment clinic in Chatsworth, Georgia. The state is among a handful with a statutory limit on the number of clinics that can be licensed.
While Congress and the Trump administration were promoting greater use of the addiction medication buprenorphine to quell the opioid epidemic, a handful of states were licensing new methadone clinics in dozens of the nation’s hardest-hit communities.
In fact, the methadone treatment industry, which began in the late 1960s, grew more in the past four years than it has in the past two decades, said Mark Parrino, president of the American Association for the Treatment of Opioid Dependence Inc., which represents methadone treatment providers.
Between 2014 and 2018, the methadone industry added 254 new clinics, according to data from the Drug Enforcement Administration. In the two decades before that, increases in the number of programs were only incremental, Parrino said. “We haven’t seen such a dramatic increase in the industry since the 1970s.”
But despite a national drumbeat for more science-based treatment for people addicted to prescription painkillers, heroin and other illicit opioids, the opioid treatment industry’s expansion has mostly gone unheralded.
Unlike buprenorphine, which can be prescribed by specially licensed practitioners and taken orally at home, or injectable Vivitrol, which can be administered by any doctor, methadone must be doled out daily at highly regulated and often very visible clinics.
Crowded parking lots, long lines and the potential for diversion of the medication have led many states to limit the number of clinics they license.
Some politicians and many in the general public have likened methadone treatment to trading one addiction for another. And certain politicians — including former New York City Mayor Rudy Giuliani, a Republican, and former Vermont governor and Democratic presidential candidate Howard Dean — have criticized use of the medication.
That’s starting to change.
“There has been an underlying stigma against methadone for so many years that the industry naturally maintains a low profile,” said Dr. Yngvild Olsen, an addiction doctor in Baltimore and board member of the American Society of Addiction Medicine. “Even now,” she said, “access to methadone is highly geographic. It depends on where you live.”
In an opioid epidemic that is killing more than 130 Americans every day, more states, including some that previously limited expansion of methadone treatment, are calling on the industry to set up new programs in opioid-plagued rural and suburban areas that lack adequate medication-assisted treatment options.
And opioid treatment companies are responding, with most new clinics offering all three FDA-approved opioid addiction medications. A major driver of the recent expansion is millions in newly available Medicaid reimbursement dollars for methadone treatment in at least 37 states and the District of Columbia.
Among the most aggressive states in seeking methadone treatment expansion have been Indiana, Maryland and New York, which have strategically sited dozens of new facilities in rural and suburban communities in the past two years. Ohio and Florida are planning major expansions this year and next.
At the same time, laws and regulations in at least six other states — Georgia, Indiana, Louisiana, Mississippi, West Virginia and Wyoming — still curtail licensing of new methadone clinics, even though people with opioid addictions in large swaths of those states live too far from the nearest methadone clinic to commute.

New York state officials, including the drug and alcohol commissioner, Arlene González-Sánchez (middle), and Lt. Gov. Kathy Hochul (third from left), attend a ribbon-cutting ceremony in Batavia, New York, for the opening of a new methadone clinic. New York is among a handful of states that are urging opioid treatment providers to set up new clinics in underserved areas.
Indiana added at least 10 new clinics in the past two years, doubling the previous number of clinics in the state. But an existing law still on the books caps future growth. To allow expansion, Ohio lifted a previous moratorium on allowing private companies to start methadone clinics in the state.
Reimbursement for methadone treatment started becoming available in the past four years in many of the 33 states and the District of Columbia where Medicaid has been expanded under the Affordable Care Act to cover low-income adults. As a result, the opioid treatment industry has the financial incentive it needs to invest in new facilities.
Remaining states that do not allow Medicaid reimbursement for methadone treatment are Alabama, Arkansas, Idaho, Illinois, Iowa, Kentucky, Louisiana, Nebraska, North Dakota, South Carolina, Tennessee, Texas and Wyoming, several of which have among the nation’s highest rates of opioid addiction and overdose deaths.
In January 2020, Medicare coverage of methadone treatment for people 65 and older is slated to begin under the recently enacted Opioid Crisis Response Act, further boosting potential revenue for opioid treatment providers.
Tightly Regulated
Methadone and buprenorphine are opioids that when taken orally eliminate withdrawal symptoms and drug cravings without producing euphoria in people who quit prescription painkillers or heroin.
Vivitrol, a 30-day injection, blocks the effects of opioids and alcohol and is not a narcotic. With less research on its outcomes, the relatively new drug is considered effective for only certain people.
The American Society of Addiction Medicine advises that all three medications be considered for any patients seeking treatment for an opioid addiction to determine which medicine will work best.
For many, only methadone will sufficiently quiet drug cravings, particularly those who have used high doses of heroin for many years and those who have used the more potent synthetic opioid fentanyl. For others, buprenorphine or Vivitrol may be the best choice.

To open a methadone clinic, companies and nonprofits must apply for a state license after demonstrating a need for the service. In states that are aggressively pursuing greater opioid treatment capacity, the need is typically established through legislative or executive initiatives and companies are asked to submit a business proposal.
“It’s entirely up to states to determine whether they have sufficient opioid treatment capacity,” Parrino said. The federal government offers no guidance. As a result, states vary widely in the number of methadone clinics that serve their residents.
Most of the clinics were established with public money starting in the 1970s when an earlier heroin epidemic ravaged major urban centers. Others were added in the last two decades, particularly in smaller towns, as the opioid epidemic took hold in rural and suburban communities.
Rhode Island, Delaware, Vermont, Maryland, Connecticut, Massachusetts and Kentucky have the largest number of clinics per capita, according to a Stateline analysis of data from the Substance Abuse and Mental Health Services Administration, known as SAMHSA.
Mississippi, Nebraska, Louisiana, South Dakota, Idaho, Arkansas and Tennessee have the fewest. Wyoming has none.
Once a state issues a license and a facility’s location is approved under local zoning ordinances, companies must seek federal approval from the DEA and SAMHSA and follow strict rules.
For example, methadone is typically provided through a plexiglass shield and kept overnight in locked containers. And patients are routinely screened to ensure they’re taking the medication and not combining it with other dangerous drugs.
Most methadone patients visit a clinic daily to take their medication while a professional observes them. They also are encouraged to attend individual and group psychosocial counseling sessions. Once stabilized, some patients can take home weekend doses, often graduating to weekly and monthly take-home dosing.
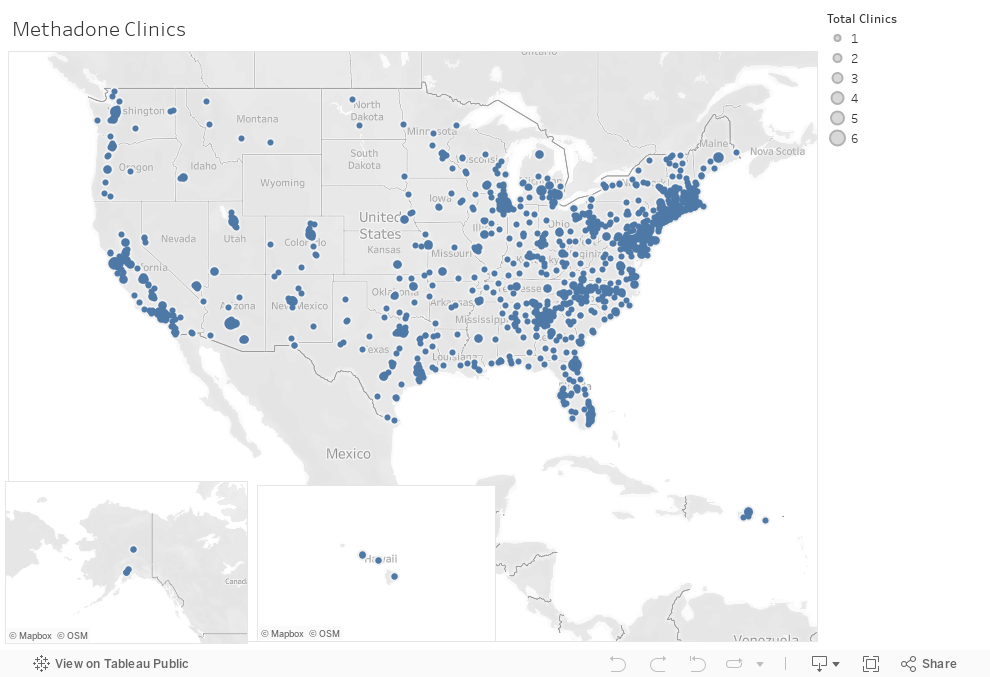
As of October, 1,611 methadone treatment programs were operating in 49 states and the District of Columbia, serving more than 380,000 patients, SAMHSA data shows. And that number is projected to grow over the next two years.
Limited Access to Other Meds
Buprenorphine, which was developed with federal funding and approved by the FDA in 2002, can be prescribed by doctors, nurse practitioners and physician assistants for 30 days at a time, picked up at a drug store and taken at home. Similar to patients taking methadone, patients who take buprenorphine are encouraged to attend individual and group counseling sessions.
Although the federal government has spent millions to support greater prescribing of buprenorphine, particularly by primary care physicians, the number of prescribers who have taken the required eight-hour DEA course, and the number of patients they are serving has been much lower than expected.
So far, most who have a buprenorphine license prescribe it for only a few patients. In most cases, primary care physicians say they obtained the license to treat existing patients with an opioid addiction and are not interested and don’t have the time to add new patients.
About 56,000 of the nation’s more than a million physicians are licensed to prescribe buprenorphine for opioid addiction, but only 112,000 patients received the medication last year, by SAMHSA’s count.
Buprenorphine is widely diverted and is sought after on the black market, particularly among active opioid users who sometimes want to abstain from the illicit drug and avoid withdrawal symptoms. Advocates for greater prescribing of the medication argue that most buprenorphine diversion is the result of the drug’s limited access through legitimate means.
Unlike methadone and buprenorphine, Vivitrol is not a narcotic and is not diverted. So far, 23,000 people are taking Vivitrol for an opioid addiction, SAMHSA has found. A long-acting injectable medication, Vivitrol was approved by the FDA in 2010 and can be prescribed and administered by any physician without obtaining a special license.
Shortages Remain
Research shows that individuals who receive addiction treatment with methadone, buprenorphine or Vivitrol are at least twice as likely to remain in treatment and achieve long-term recovery as those who receive addiction treatment without medication.
Despite the scientific evidence, only 1 in 10 people with an opioid addiction receive addiction treatment that includes those medications. About the same number of people receive addiction treatment without medications, often because none are available in their communities.
Although many people with an opioid addiction are not interested in quitting, those who do want to quit are often unable to find treatment in their community or can’t afford it.
“There’s no question that better access to methadone maintenance would save lives,” said Andrew Kolodny, who co-directs opioid treatment research at Brandeis University. “But for an addiction epidemic that is disproportionately rural and suburban, an intervention that relies on people visiting a clinic every day isn’t the best option. Buprenorphine would be better, but it’s not growing quickly enough.”
