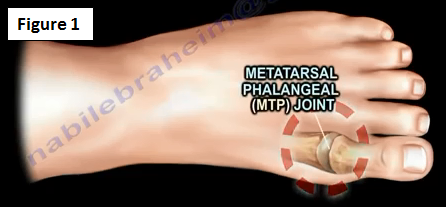
Turf toe is a hyperextension dorsiflexion injury of the big toe's first MTP joint (Figure 1). This injury tears the insertion of the plantar plate from the proximal phalanx which leads to an incompetent plantar sesamoid complex (Figure 2). Turf toe is seen more involving contact sports that are played on rigid surfaces.

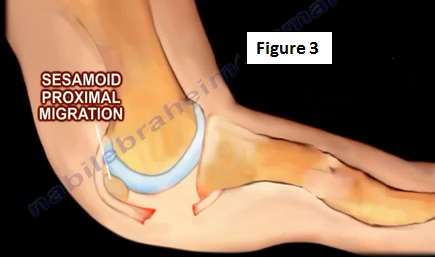
The big toe (MTP joint) is positioned in hyperextension and the forefoot is fixed to the ground. With axial load to the heel, the plantar plate sesamoid complex tears. The sesamoid bone may fracture or proximally migrate (Figure 3). An occult fracture of the proximal phalanx may be present.
When you classify these injuries, they can be a sprain, partial tear, or a complete tear.
Injuries
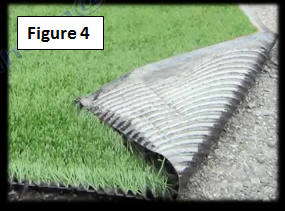
There are many factors implicated with an increased incidence of turf toe. A combination of multiple factors associated with turf toe includes an increased hardness of the artificial turf and increased shoe flexibility (Figure 4). Factors that are associated with the patient developing turf toe are the weight of the athlete/patient, age, the type of sport being played and factors associated with the foot itself. Turf toe injuries occur with a lot of different sports; however they are common with football players.
Clinical Picture
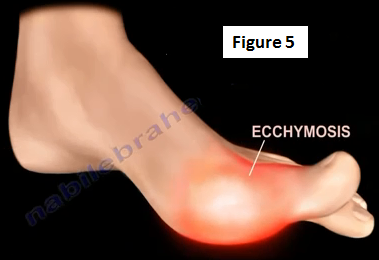
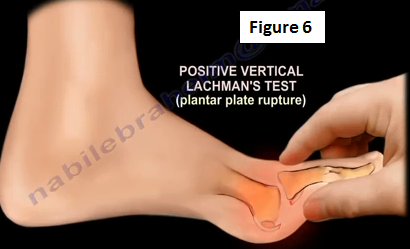
The patient will present with pain, swelling and an inability to "push off" with the big toe. The patient will have plantar swelling, tenderness and ecchymosis (Figure 5). The vertical Lachman's test will be positive (Figure 6). Varus and valgus instability will be present. The physician should always compare the injured foot to the other side.
An x-ray will need to be obtained. Either a fracture or proximal migration of the sesamoid bone will be seen. If seen on an AP view x-ray, this means that there is complete rupture of the plantar plate. The sesamoid bone will not move under fluoroscopy with range of motion of the first MTP joint.
Treatment
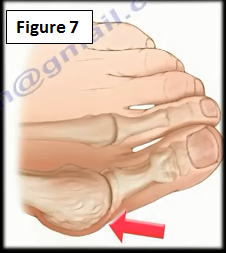
These injuries have the potential to become a chronic problem. Most athletes and coaches perceive this injury as a small, trivial injury. Most athletes return to sports without sufficient time for healing and recovery. Approximately 50% of these patients will complain of persistent symptoms, such as stiffness of the big toe or hallux valgus deformity after more than five years after the injury occurred (Figure 7). This will lead to chronic disability and prevent the athlete from competing.
Most of these injuries can be treated conservatively with ice, rest, taping, and orthotics (rigid Morton's extension) (Figure 8). In the most severe cases, a boot or a cast will be worn for a few weeks followed by therapy for motion.

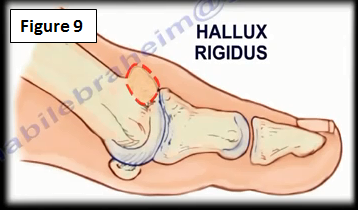
Surgery for repair is rare. Surgery is done if there is failure of conservative treatment. Surgery is also done if there is a Grade III tear (complete tear of the plate). The physician repairs the plantar plate to the proximal phalanx through a plantar approach. The sesamoid bone may be exercised partially or completely if it is fractured. The return to play is usually about 3-4 months after surgery. The late sequela is hallux rigidus, which may need rigid Morton's extension or surgery, called cheilectomy (Figure 9).
For more information on athletic injuries and toe pain follow the links below:
https://www.youtube.com/watch?v=BkGVWTeJTqs
https://www.youtube.com/watch?v=c6biKrtwoY0
https://www.youtube.com/watch?v=7jFEMY7oCc0
https://www.youtube.com/watch?v=G2nP0D024X8
https://www.youtube.com/watch?v=COhxfTGohMg
https://www.youtube.com/watch?v=pex6DIx8Cek
https://www.youtube.com/watch?v=LQuc05F4-B8
https://www.youtube.com/watch?v=SrOlhCF38EY
https://www.youtube.com/watch?v=6H5henaYCe0
For more topics, visit my YouTube Channel:https://www.youtube.com/user/nabilebraheim